Teagan’s CDH Story

In February of 2024, the excitement of finding out we were having another girl was replaced with disbelief and sadness. Our baby girl had been diagnosed with Congenital Diaphragmatic Hernia (CDH).
After confirmation from a local specialist, we were referred to our team in Madison, led by our pediatric surgeon and Maternal Fetal Medicine (MFM) doctor. There were a lot of ultrasounds, consultations, and conversations about genetics, CDH, and our options. A fetal MRI then diagnosed Teagan with a severe case — lung volume of 26% or less. At that stage, she had less than a 50% chance of survival.
We faced an impossible decision: terminate the pregnancy, continue as is, or pursue an in-utero surgery called Fetoscopic Endoluminal Tracheal Occlusion (FETO). It didn't take long to know what we needed to do — to give Teagan the best chance of survival, and to give ourselves the chance to meet her.
The FETO procedure required us to temporarily relocate our family to Madison at 29 weeks. Our pediatric surgeon, Dr. Inna Lobeck, placed a tiny balloon, just 1mm, the size of a grain of rice — in Teagan's throat to help her lungs fill with fluid and grow. After the balloon was placed, I had ultrasounds twice a week to track it and monitor fluid levels. Twice, I had to have amnioreductions to remove excess fluid, about eight liters total, to help keep Teagan in as long as possible.
At 35 weeks, Dr. Lobeck completed the second half of the FETO procedure, popping the balloon with a needle. The clock started. We prayed and hoped Teagan would stay in as long as possible. We had a planned c-section at 38 weeks, but Teagan arrived on her own time at 37 weeks and 2 days.
At birth, she was immediately resuscitated and transferred to the NICU. At just 2 days old, Teagan had her CDH corrective surgery. We learned then that nearly every abdominal organ, except her bladder and one kidney, had been in her chest cavity, and she had less than 10% of her diaphragm. Because of the FETO balloon, her lungs had grown well enough that even with her liver up, the impact was less severe. The surgery was a success.

On day three, an unplanned return to the OR led to Teagan developing Pulmonary Hypertension. After trying several ventilator options, Nitric Oxide saved her from needing ECMO, the highest form of life-saving support.
Over the following weeks in the NICU, Teagan graduated through levels of respiratory support and began working with Speech, Occupational, and Physical therapists. Once she was breathing on room air, we tried bottle feeding and for about a week, it worked. But we couldn't meet volume goals, and severe reflux set in, leading to an oral aversion. Teagan needed a g-tube, and after careful conversations with her doctors, she also had a Nissen fundoplication to address the reflux. Both surgeries were successful.
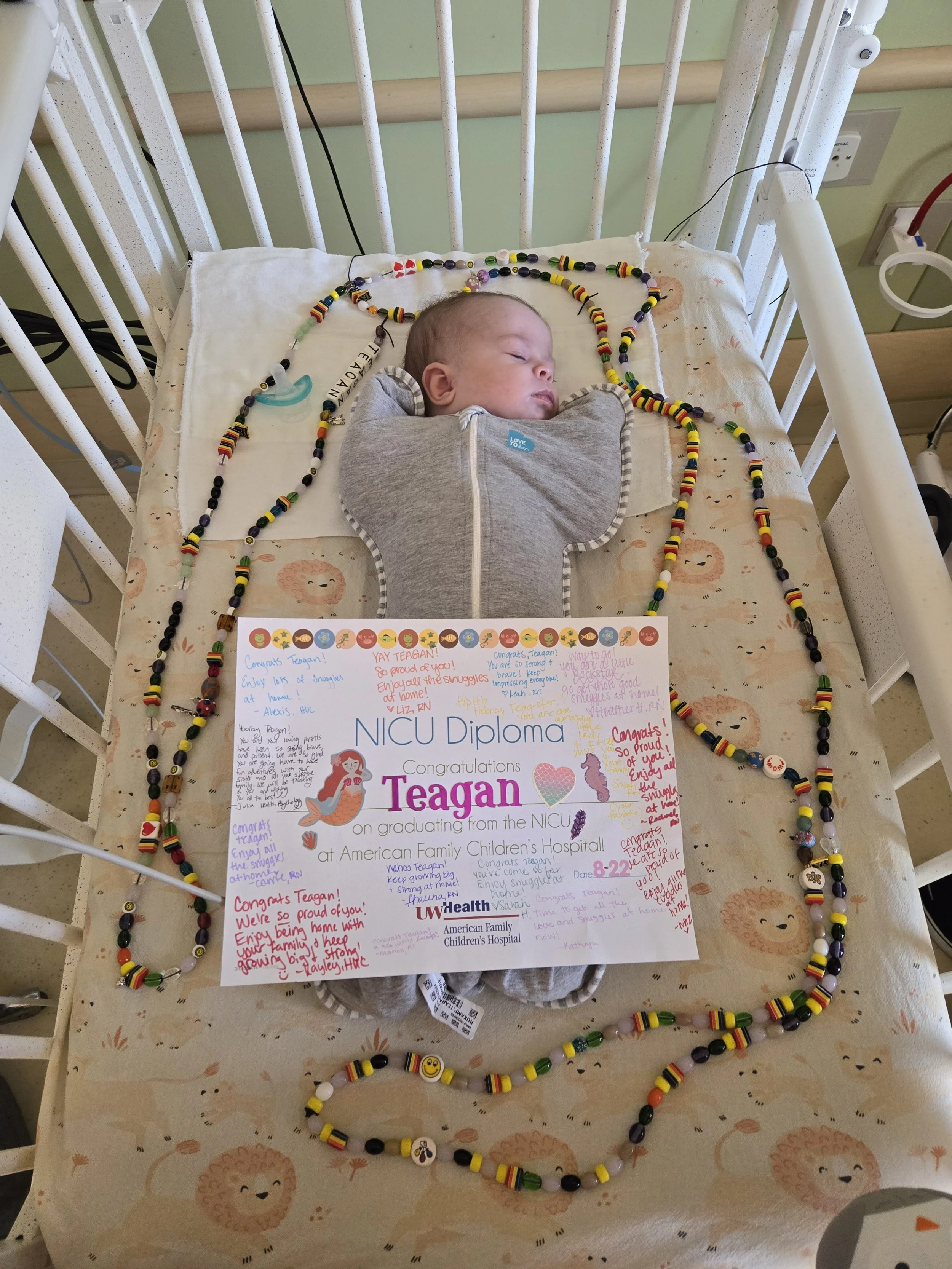
Three days later, after 79 days in the NICU and five and a half months living in Madison, we finally went home.
Since then, Teagan has worked with Speech, Occupational, Physical, and Birth to Three therapies — and now she is completely eating by mouth. Teagan is our little miracle. We are so grateful for our team at UW Health / American Family Children's Hospital in Madison.
Do not lose hope. These babies are so resilient. The rollercoaster is worth it.